Whiplash and Whiplash Associated Disorder (WAD)
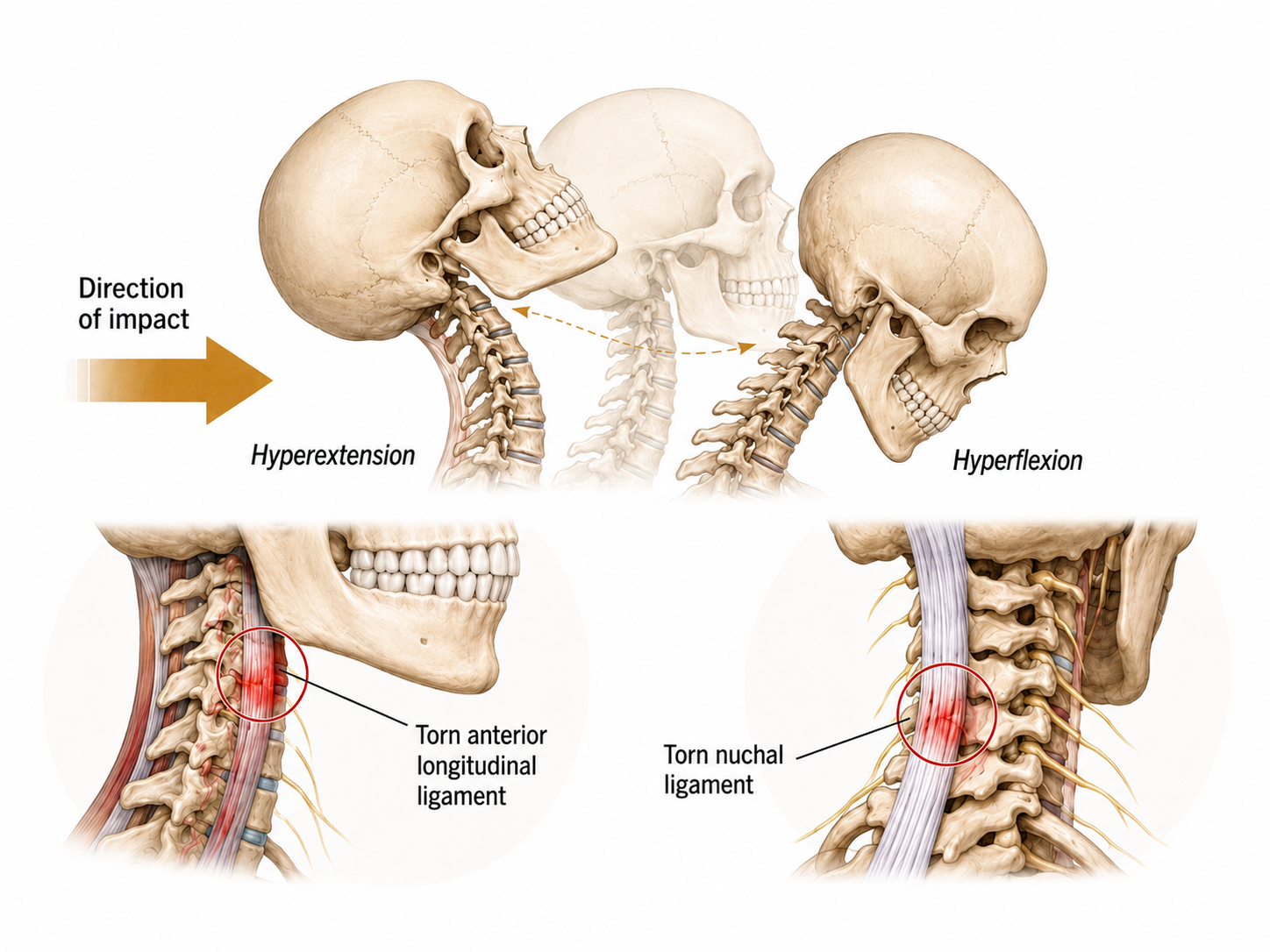
Most people think whiplash only happens in a serious car crash. It is more accurately described as an acceleration-deceleration force on the neck, and that can come from a rear-end or side-impact collision, a slip on the ice, a hit from behind in hockey, soccer, football, or rugby, or even a minor-looking fall off a bike. These forces can irritate or injure the muscles, ligaments, and joints of the neck and nearby spine. Sometimes they cause no injury or pain at all.
One detail that often gets missed: whiplash can involve the front of the neck. Anterior neck pain is common after these injuries, and restoring control and strength in the front neck muscles is often central to recovering well.
A proper diagnosis takes a thorough evaluation, and sometimes imaging. The injury is then classified, because the grade shapes everything that follows.[1]
The Five Grades of WAD
Whiplash Associated Disorder describes neck pain and stiffness after trauma to the head and neck. Symptoms can appear immediately or come on hours to days later, and they vary widely from person to person. The grade is matched to your specific signs and symptoms.[1]
Grade 0
You were in an incident, but you have no neck pain, no stiffness, and no physical signs.
Grade I
Neck pain, stiffness, or tenderness only, with no other physical signs. There is usually no sign of major damage to muscle, disc, or joint, and little disruption to daily life. You may feel tenderness through the neck, shoulder, and jaw muscles and some stiffness, but without neurological complaints or signs of serious structural injury. Imaging is often not needed. Staying as active as tolerated and avoiding immobilizing the neck is important here, though an assessment confirms the diagnosis.
Grade II
Reduced range of motion and point tenderness in the neck. There are no signs of major damage, but the pain interferes with daily activities and limits head and neck movement. Signs of serious structural injury or nerve root compression are rare, though imaging may be used to be certain.
Grade III
This is where severity increases. Neck complaints come with neurological signs such as reduced deep tendon reflexes, weakness, and sensory changes. Neurological signs or symptoms are always present. If you have weakness, or numbness and tingling, this needs prompt assessment. Provocation tests can help assess whether a nerve root is involved. Severe arm or neck pain with major neurological deficits from the moment of injury, or symptoms that are worsening, may require urgent medical imaging such as CT or MRI to define the extent of the injury.
Grade IV WAD means neck pain with signs of major structural injury, such as a fracture or dislocation, and possible injury to the spinal cord. Possible signs include severe pain, neurological symptoms, inability to support the head comfortably, or a feeling of instability.
This must be managed at a hospital. If you suspect it, go to the nearest emergency department immediately.
What Is the Outlook?
- For WAD 0 to II, the outlook is usually good. Grade I symptoms commonly begin improving within a few days, though timelines vary with the person and history. If symptoms persist past a few days, have it assessed.
- Chronic or recurrent pain can occur with WAD I and II. The pain comes and goes with flares, usually driven by repetitive load, sustained positions, stress, or underlying weakness rather than ongoing damage. An active rehabilitation approach is the right tool here.[3][5]
- WAD III often needs a broader team. When neurological symptoms are involved, an orthopaedic surgeon or neurologist may help guide management. Some Grade III cases are managed conservatively, provided the clinician is experienced with this kind of injury and your symptoms are improving in the first few visits.
- WAD IV requires emergency medical care and specialist assessment. Immobilization and, in some cases, surgical stabilization may be required when fracture, dislocation, or spinal cord risk is present. Go to the nearest emergency department if you believe you have an injury this severe.
For most whiplash (WAD I to III without instability), prolonged immobilization and soft collars tend to slow recovery rather than speed it. Staying gently active within comfort, restoring movement early, and progressively loading the neck is the better-supported path. The exception is a confirmed unstable or Grade IV injury, which is managed very differently.
How Is Whiplash Treated?
The aim is to restore safe, comfortable mobility and capacity for WAD 0 to III. If WAD IV is suspected, emergency immobilization and hospital management take priority. For WAD I to III, conservative management may include:[2][4][6]
- Hands-on care. Joint manipulation and mobilization, soft tissue and fascial techniques, and medical acupuncture, matched to your stage and irritability.
- Neck stability and strengthening exercises. Very important, including the front neck muscles, but only once the correct diagnosis is established so symptoms are not aggravated.
- Position habits and movement variety. Helpful for preventing flares, again best started after an accurate diagnosis.
- Pain medication, when appropriate. Discuss options with your physician or pharmacist.
Return to a professional if the pain worsens, if it persists beyond three to five weeks, or if you develop new or worsening numbness, weakness, pins and needles, or symptoms travelling into an arm or hand.
To drive, cycle, or ride a motorcycle safely, you must be able to check blind spots quickly and comfortably. Avoid driving if your neck movement is too limited to do that safely, or if pain, dizziness, arm symptoms, medication, or post-accident symptoms affect your control.
Whiplash recovers best when it is classified accurately and managed actively from the start. If you have been in a collision or a fall, a thorough assessment sets the right course. Call the clinic at 647-560-4495.
Book an Assessment at ONE80References
All references link directly to PubMed. Tap a citation number in the article to jump here. Tap the arrow beside a reference to return to where you were reading.
- Spitzer WO, et al. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders. Spine. 1995;20(8 Suppl):1S-73S. pubmed.ncbi.nlm.nih.gov/7604354 ↩
- Sterling M. Physiotherapy management of whiplash-associated disorders (WAD). J Physiother. 2014;60(1):5-12. pubmed.ncbi.nlm.nih.gov/24856935 ↩
- Ritchie C, Sterling M. Recovery pathways and prognosis after whiplash injury. J Orthop Sports Phys Ther. 2016;46(10):851-861. pubmed.ncbi.nlm.nih.gov/27594661 ↩
- Southerst D, et al. Is exercise effective for the management of neck pain and associated disorders or whiplash-associated disorders? A systematic review by the OPTIMa Collaboration. Spine J. 2016;16(12):1503-1523. pubmed.ncbi.nlm.nih.gov/24534390 ↩
- Michaleff ZA, et al. Comprehensive physiotherapy exercise programme or advice for chronic whiplash (PROMISE): a randomised controlled trial. Lancet. 2014;384(9938):133-141. pubmed.ncbi.nlm.nih.gov/24703832 ↩
- Sterling M, et al. Best evidence rehabilitation for chronic pain part 4: neck pain. J Clin Med. 2019;8(8):1219. pubmed.ncbi.nlm.nih.gov/31443149 ↩