Myofascial Pain and Trigger Points: The Knots in Your Neck
Almost everyone has felt them: the tight, tender bands across the top of the shoulders and into the neck that you instinctively reach up to squeeze. These are often described clinically as myofascial trigger points, and the broader pattern of pain they create is called myofascial pain. They are one of the most common findings in necks and shoulders, and they show up constantly alongside the other conditions in this series.[2]
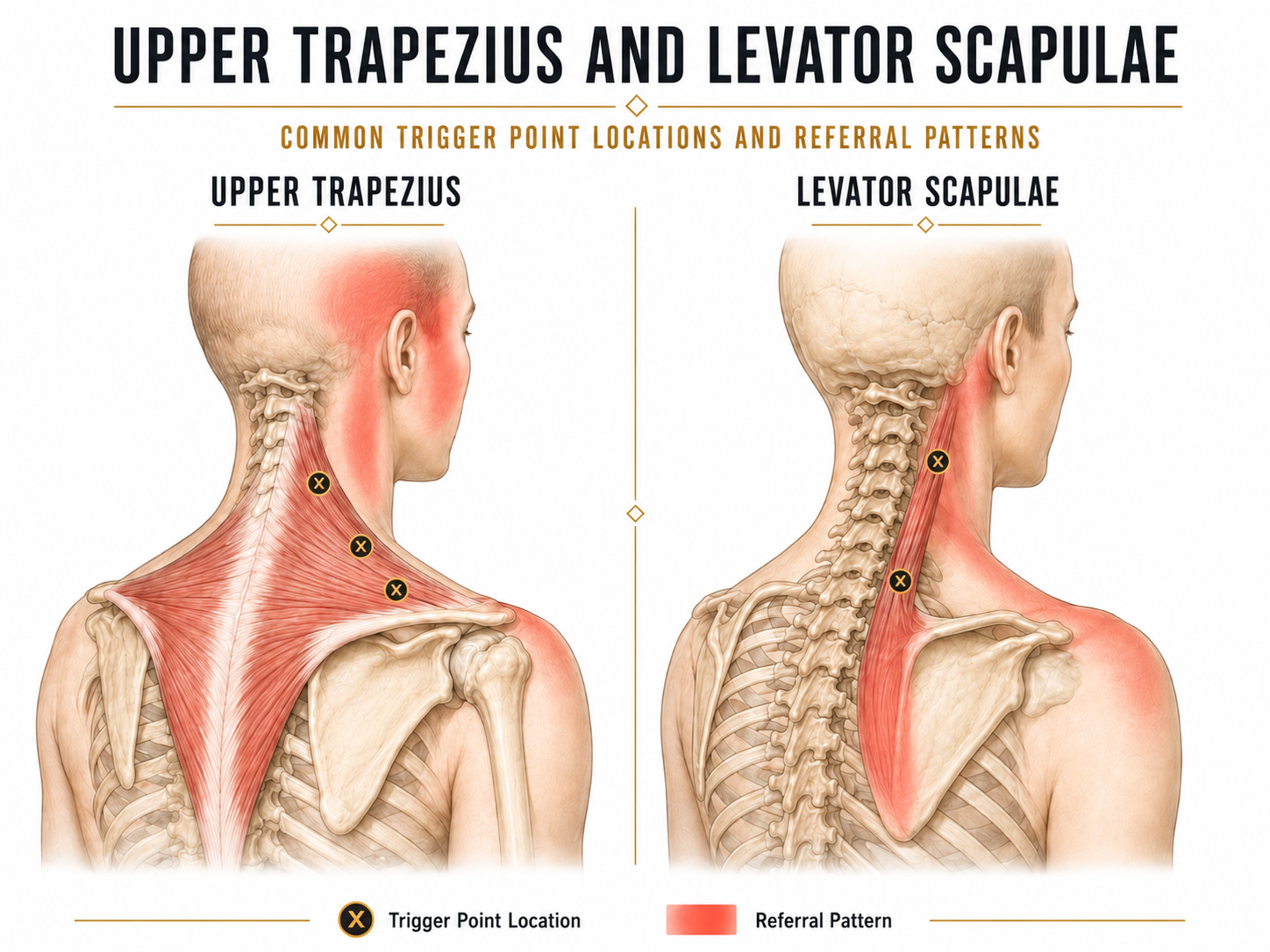
A trigger point is commonly described as a tender, taut band within a muscle, a small region that has become sensitive and overactive. Press on one and it often feels like a firm nodule, and it can reproduce a familiar ache. The muscles around the neck and shoulder, especially the upper trapezius and levator scapulae, are classic homes for them.[1]
A common feature of an active trigger point is referred pain. A knot in the upper trapezius can send pain up into the temple and behind the eye, and a knot in levator scapulae can drive that nagging ache at the inner corner of the shoulder blade. This is why people are often surprised to learn their headache or shoulder-blade pain is actually coming from a muscle in the neck. It also explains why rubbing only the spot that hurts sometimes does not help, the real source can be elsewhere.
Why These Knots Keep Company
Trigger points rarely exist in isolation. They tend to develop when a muscle is overloaded, held in a shortened or braced position, or asked to work constantly without rest. That description fits almost every other neck condition. A neck that hurts from mechanical strain, a guarded neck after whiplash, or a stiff, arthritic neck all create conditions that can perpetuate trigger point sensitivity. They are frequently the symptom layer sitting on top of a deeper driver.
Stress and breathing deserve special mention. When we are stressed we brace, elevate the shoulders, and breathe into the chest and neck rather than the belly. The upper trapezius and the accessory breathing muscles of the neck then work overtime, all day, which is a near-perfect recipe for persistent trigger points.
The Symptoms
- Tender, rope-like bands across the neck and the top of the shoulders.
- A deep, aching pain rather than a sharp one, that often refers to a predictable spot.
- Referred headaches, particularly tension-type headaches that climb from the neck into the head.
- A feeling of constant tightness that returns soon after stretching or massage, because the underlying driver has not changed.
What Actually Releases Them
Trigger points respond well to hands-on care, but lasting relief comes from also addressing why they formed.[3][4][5]
- Soft tissue and fascial techniques. Targeted manual work and instrument-assisted soft tissue therapy can release the taut bands and calm the referral pattern. Active Release and related techniques are well suited to this.
- Medical acupuncture and dry needling. Needling into an active trigger point can reduce sensitivity, with supportive evidence for short-term relief of neck-related trigger point pain.[3][4] More on our acupuncture approach.
- Strengthening and endurance work. The step most people skip. Muscles that have the endurance to do their job stop being chronically overloaded. Building capacity in the neck and upper-back stabilizers is what stops the knots from simply reforming.[6] See the neck mobilization and stability program.
- Posture variety and breathing retraining. Changing positions often, and restoring relaxed diaphragmatic breathing, removes the constant background load that keeps trigger points alive.
If you have noticed that massage feels wonderful but the tightness is back within a day or two, this is why. Releasing a trigger point treats the symptom layer. Unless you also reduce the load that helped create it, through strengthening, better position habits, and calmer breathing, the muscle often returns to its overworked state. Release plus capacity is what makes the relief more likely to last.
Trigger points often respond well to the right combination of release, strengthening, breathing, and load management. A focused assessment finds the real driver so the relief is more likely to last. Call the clinic at 647-560-4495.
Book an Assessment at ONE80References
All references link directly to PubMed. Tap a citation number in the article to jump here. Tap the arrow beside a reference to return to where you were reading.
- Fricton J. Myofascial pain: mechanisms to management. Oral Maxillofac Surg Clin North Am. 2016;28(3):289-311. pubmed.ncbi.nlm.nih.gov/27475508 ↩
- Cerezo-Tellez E, et al. Prevalence of myofascial pain syndrome in chronic non-specific neck pain: a population-based cross-sectional descriptive study. Pain Med. 2016;17(12):2369-2377. pubmed.ncbi.nlm.nih.gov/28025371 ↩
- Navarro-Santana MJ, et al. Effectiveness of dry needling for myofascial trigger points associated with neck pain symptoms: an updated systematic review and meta-analysis. J Clin Med. 2020;9(10):3300. pubmed.ncbi.nlm.nih.gov/33066556 ↩
- Gattie E, et al. The effectiveness of trigger point dry needling for musculoskeletal conditions by physical therapists: systematic review and meta-analysis. J Orthop Sports Phys Ther. 2017;47(3):133-149. pubmed.ncbi.nlm.nih.gov/28158962 ↩
- Cagnie B, et al. Evidence for the use of ischemic compression and dry needling in the management of trigger points of the upper trapezius in patients with neck pain: a systematic review. Am J Phys Med Rehabil. 2015;94(7):573-583. pubmed.ncbi.nlm.nih.gov/25768071 ↩
- Gross A, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2015;1:CD004250. pubmed.ncbi.nlm.nih.gov/25629215 ↩