Cervical Spondylosis: Understanding the Aging Neck
Cervical spondylosis is the medical term for degenerative osteoarthritis of the neck. It describes the wear and tear that accumulates in the vertebrae and the discs between them over the years. The name sounds serious, and it can be unsettling to read on an imaging report, but for many people the reality is far more reassuring than the terminology suggests.
Degenerative changes in the neck are a normal part of aging, and they are very often painless. On MRI, a large share of people with no neck pain at all show disc degeneration, bulges, and arthritic changes, and the proportion climbs steadily with each decade.[2][3] In other words, the changes on the scan are frequently not the source of the pain. This is why I treat the person in front of me, not the picture.
What Is Actually Happening?
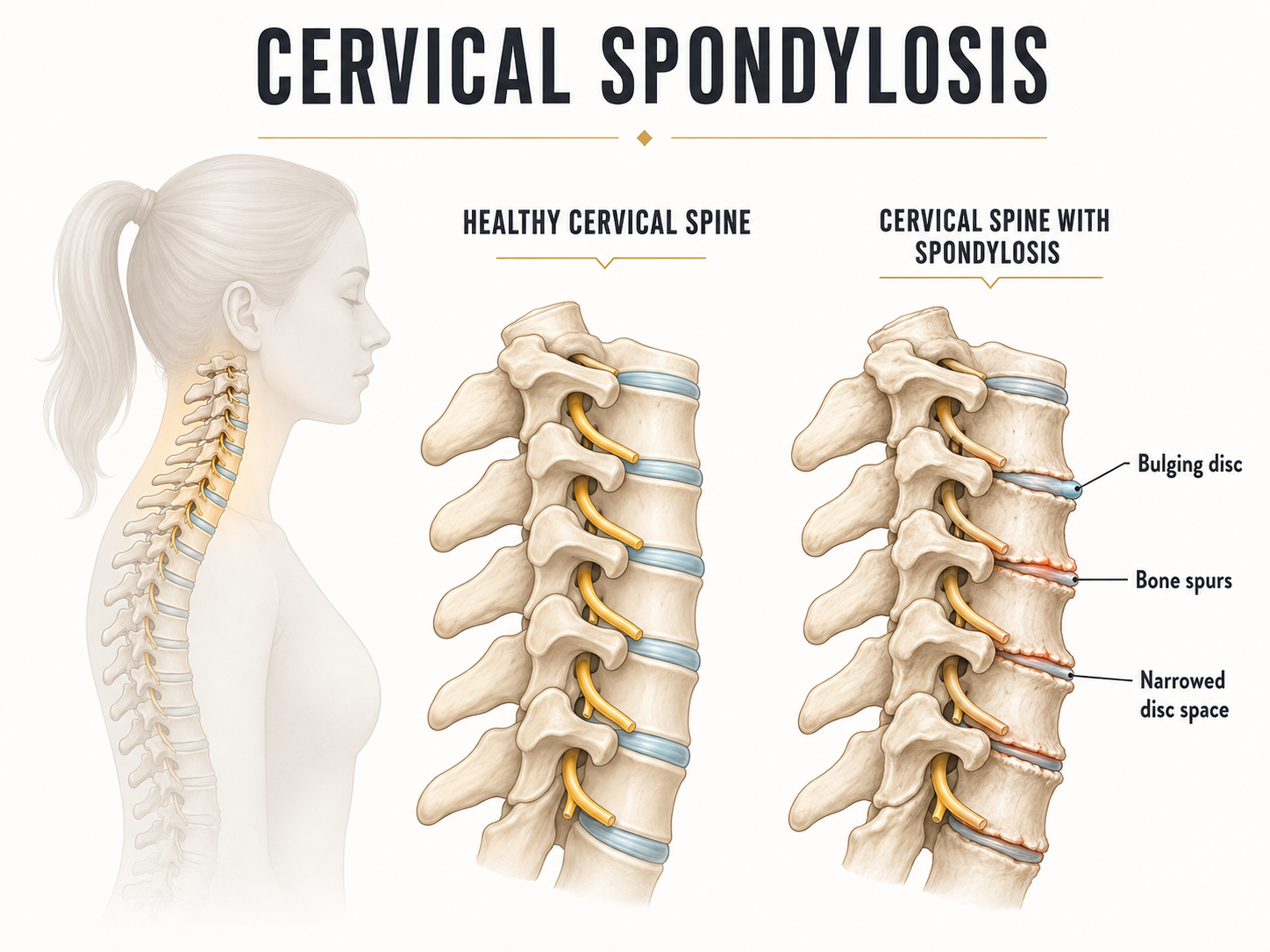
With time, the discs lose some height and hydration, the vertebral bodies can develop small bony spurs (osteophytes), and the joints of the neck show the same kind of arthritic change that other joints do. This is the cervical spine adapting to decades of use.[1]
Patients with spondylosis often feel pain at the end ranges of movement, and in some cases the changes can narrow the space where nerves exit, contributing to cervical radiculopathy. For most people, though, spondylosis is a background finding rather than a disabling problem, and the priority is preventing further stiffening and deconditioning.
What Are the Symptoms?
- Stiffness, especially in the morning or after long periods in one position.
- Pain at the end of range, particularly with rotation or looking up.
- A sense of grinding or clicking with movement, which is common and usually not a cause for concern on its own.
- Occasionally, referred symptoms if degenerative changes irritate a nerve, in which case symptoms can travel toward the arm.
For most people, spondylosis is not dangerous, but a few symptoms warrant attention because they can signal nerve or spinal cord involvement:
- Progressive numbness, tingling, or weakness in an arm or hand
- Clumsiness of the hands, changes in handwriting or buttoning, or unsteadiness when walking
- Pain that is steadily and progressively worsening, or that comes with feeling unwell, fever, or unexplained weight loss
These are uncommon, but they are worth checking promptly rather than waiting.
Why Mobility and Strength Are the Priority
Here is the key principle: with a degenerative neck, you cannot reverse the wear, but you have a great deal of influence over how it feels and functions. Keeping the neck mobile and strong is one of the most important components of long-term success.[5][6]
A stiff, deconditioned neck around arthritic joints tends to be a sore neck. A mobile, well-supported neck around the very same joints often feels fine. Movement keeps the joints nourished and the range available, and strengthening the deep neck flexors and stabilizers gives those joints the support they need to tolerate daily life comfortably. Our neck mobilization and stability program is designed exactly for this.
How Is It Managed?
The aim is comfortable movement and lasting capacity, not chasing the scan.[6]
- Mobility work to maintain and restore range, especially the ranges that have quietly been lost.
- Progressive strengthening of the deep neck flexors and the stabilizers of the neck and upper back.
- Hands-on care, including mobilization, soft tissue and fascial techniques, and medical acupuncture, to ease pain and improve movement so you can exercise comfortably.
- Attention to posture variety, sleep, and stress, since all three influence how an arthritic neck feels day to day. See our neck and sleep article.
If your report mentions degeneration, disc bulges, osteophytes, or arthritis, take a breath. These findings are common in people your age who have no pain whatsoever.[2][3] The presence of wear does not mean a future of pain, and it does not mean you are fragile. A capable, gradually loaded neck is the goal, and for many people it is very achievable.
A degenerative neck does not have to be a painful neck. A focused assessment and the right mobility and strengthening plan keep you moving comfortably for the long run. Call the clinic at 647-560-4495.
Book an Assessment at ONE80References
All references link directly to PubMed. Tap a citation number in the article to jump here. Tap the arrow beside a reference to return to where you were reading.
- Theodore N. Degenerative cervical spondylosis. N Engl J Med. 2020;383(2):159-168. pubmed.ncbi.nlm.nih.gov/32640134 ↩
- Nakashima H, et al. Abnormal findings on MRI of the cervical spine in asymptomatic subjects: a study of 1211 volunteers. Spine. 2015;40(6):392-398. pubmed.ncbi.nlm.nih.gov/25584950 ↩
- Brinjikji W, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811-816. pubmed.ncbi.nlm.nih.gov/25430861 ↩
- Kuijper B, et al. Cervical collar or physiotherapy versus wait and see for recent onset cervical radiculopathy: RCT. BMJ. 2009;339:b3883. pubmed.ncbi.nlm.nih.gov/19812130 ↩
- Gross A, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2015;1:CD004250. pubmed.ncbi.nlm.nih.gov/25629215 ↩
- Bier JD, et al. Clinical practice guideline for physical therapy assessment and treatment in patients with nonspecific neck pain. Phys Ther. 2018;98(3):162-171. pubmed.ncbi.nlm.nih.gov/29228289 ↩