Shoulder Pain: Causes, Treatment and Recovery
Shoulder pain is one of the most common reasons people come to ONE80 Health and one of the most mismanaged conditions in general practice. People receive a diagnosis of 'rotator cuff' or 'bursitis,' are given a cortisone injection, handed a generic exercise sheet, and sent home without a clear understanding of what's actually driving their pain or how to get better.
This guide is the full picture. Whether you've woken up with shoulder pain for the first time or you've been managing a chronic issue for months, this post will help you understand what's going on, what good care looks like, and what you can do to support your own recovery.
Understanding the Shoulder Complex
What most people call 'the shoulder' is actually four joints working as a single coordinated system:

Muscles of the shoulder

The Glenohumeral Joint
The ball-and-socket joint between the head of the humerus and the glenoid cavity of the scapula. The primary movement joint and the most commonly injured. Unlike the hip, where the femoral head is deeply seated, the humeral head sits on the glenoid like a golf ball on a tee. Stability comes almost entirely from the surrounding muscles, ligaments, and labrum, which is why muscular health and neuromuscular control are critical here.
The Acromioclavicular (AC) Joint
Where the clavicle meets the acromion at the top of the shoulder. Commonly injured in contact sports through a direct fall or impact. Graded sprains (I–III) determine whether conservative or surgical management is appropriate.
The Sternoclavicular Joint
Where the clavicle meets the sternum. Often overlooked in shoulder assessments, but its mobility directly affects how the clavicle and scapula move during arm elevation.
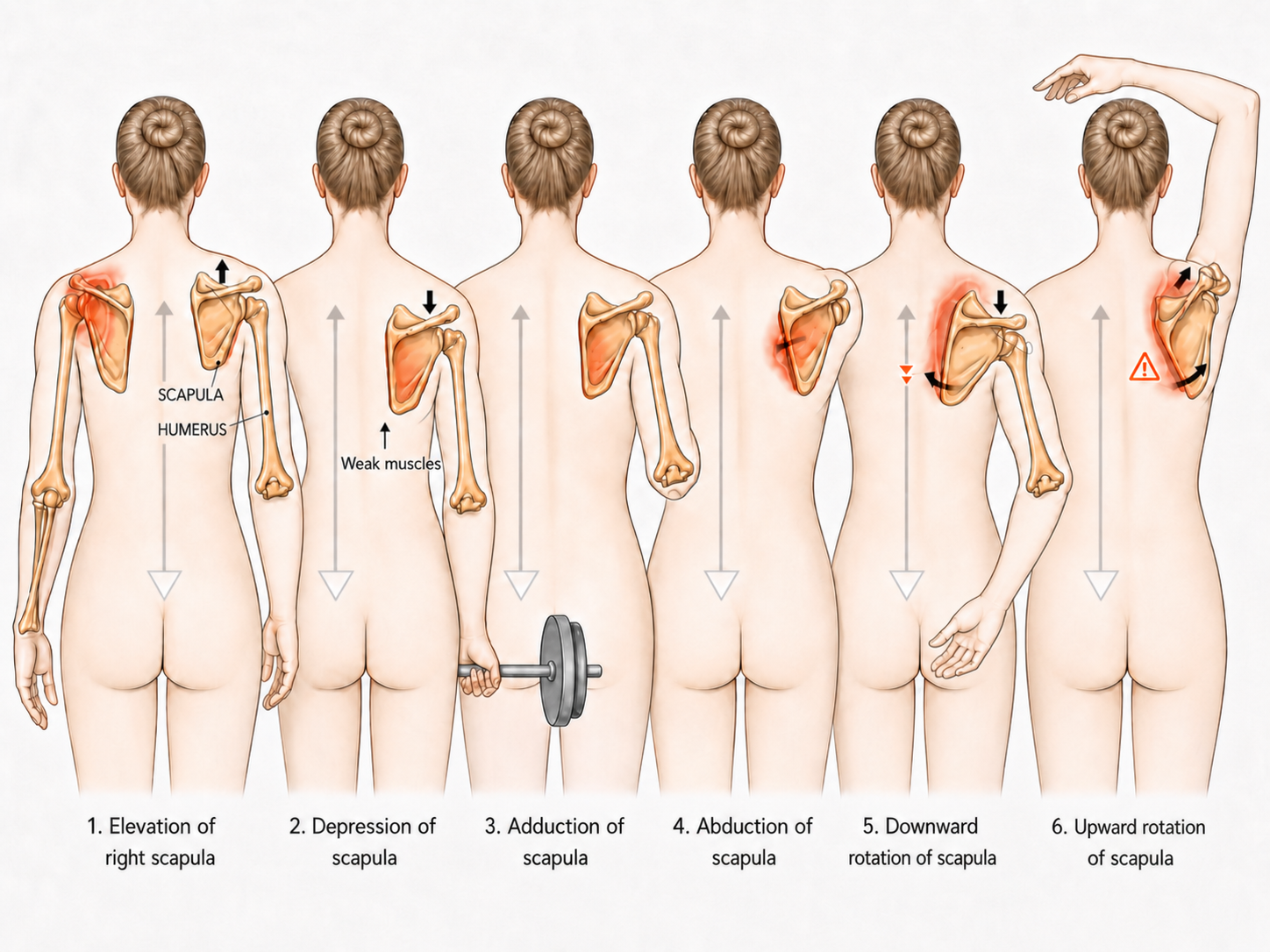
The Scapulothoracic Interface
Not a true anatomical joint, but a critical functional one, the scapula gliding against the posterior ribcage. For every degree the arm elevates, the scapula must rotate and tilt in a precise, coordinated sequence. Disruption of this movement pattern is one of the most common and underdiagnosed drivers of shoulder pain.
Scapulohumeral Rhythm
The coordinated movement between the glenohumeral joint and the scapulothoracic interface during arm elevation is called scapulohumeral rhythm, approximately a 2:1 ratio of glenohumeral to scapulothoracic motion. The first 30 degrees of shoulder abduction is primarily glenohumeral; beyond that, both joints move simultaneously. When this rhythm breaks down, due to muscle weakness, tightness, poor thoracic mobility, or fatigue, the subacromial space narrows, the rotator cuff is placed under excessive load, and tissue breakdown begins. [2]
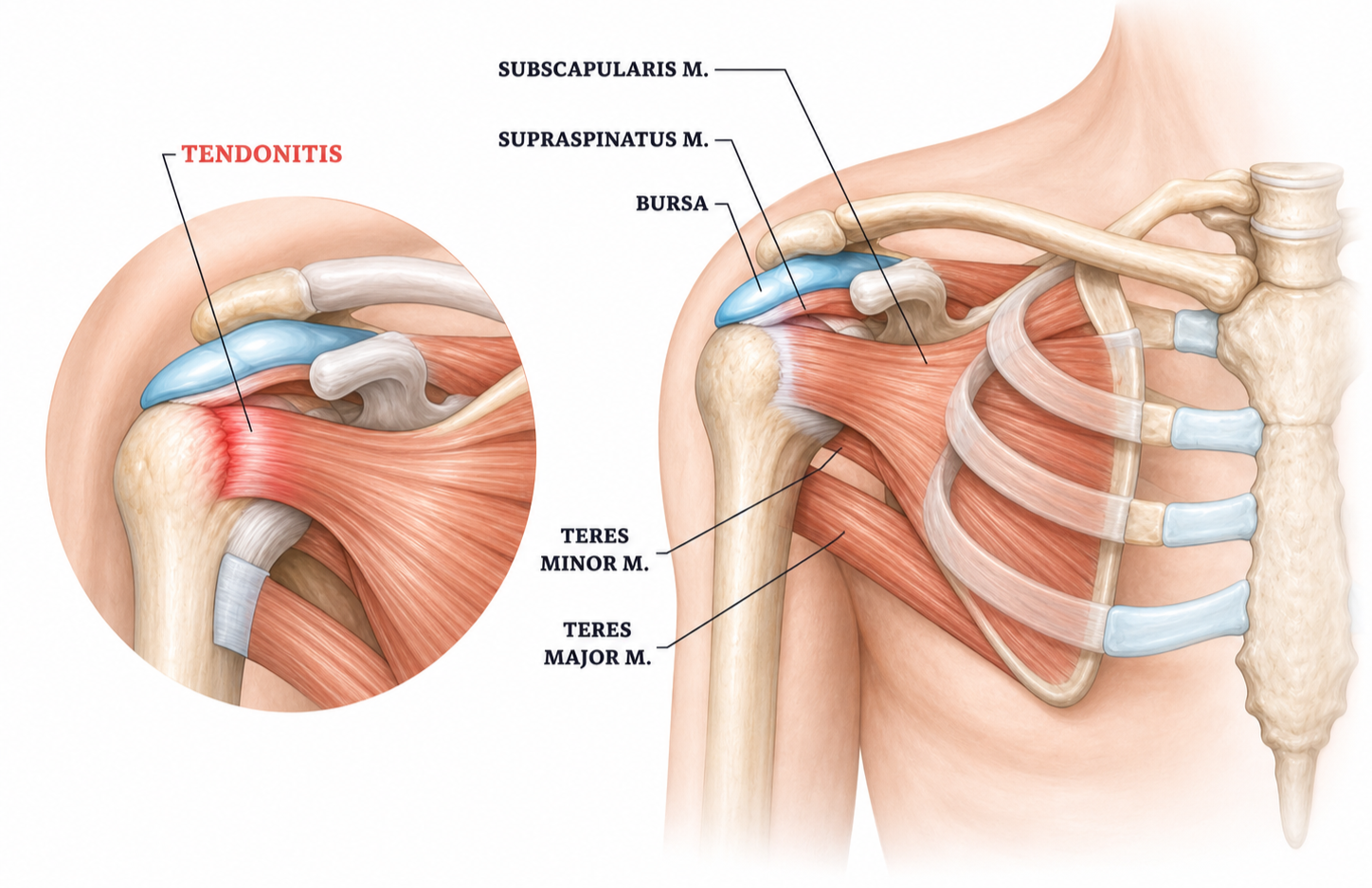
The Rotator Cuff
Four muscles form the rotator cuff, supraspinatus, infraspinatus, subscapularis, and teres minor. Their tendons merge into a continuous hood over the humeral head. Their primary function is not to produce movement, but to keep the humeral head centred in the joint socket while the larger muscles (deltoid, pectoralis major, latissimus dorsi) generate force. A compromised rotator cuff means a compromised foundation for every shoulder movement.
The Role of the Core and Kinetic Chain
The shoulder is the distal end of a kinetic chain that begins at the feet. Power, stability, and load transfer move from the ground upward through the ankle, knee, hip, lumbar spine, and thoracic spine before reaching the glenohumeral joint. A weak core, restricted hip mobility, or a stiff thoracic spine all increase demand on the shoulder, which is why comprehensive shoulder rehabilitation always includes assessment and treatment of the full kinetic chain.
What Causes Shoulder Pain? The Four Most Common Conditions
Most shoulder pain falls into one of four categories. Understanding which one applies to you is the first step toward managing it correctly because the right approach for a frozen shoulder is very different from the right approach for an unstable labrum.
Rotator Cuff Problems: Impingement, Tendinosis, and Tears
Rotator cuff pathology is the most common category of shoulder pain in clinical practice. It includes a spectrum from early-stage impingement through to full-thickness tears, with age over 50 and overhead occupational loading identified as the strongest modifiable risk factors. [5]
Impingement Syndrome

Impingement occurs when the supraspinatus tendon and subacromial bursa become compressed between the humeral head and the undersurface of the acromion during arm elevation. This typically happens when poor scapular mechanics or loss of rotator cuff neuromuscular control allow the humeral head to migrate superiorly, narrowing the subacromial space on every repetition of every overhead movement. Symptoms include a painful arc between 60 and 120 degrees of abduction, pain with overhead reach, and difficulty sleeping on the affected side.
Tendinosis
Where tendinitis refers to acute inflammation, tendinosis describes chronic degenerative changes within the tendon tissue itself, a structural breakdown from repetitive loading without adequate recovery. The current clinical practice guideline on rotator cuff tendinopathy emphasises that tendinosis responds poorly to anti-inflammatory approaches alone and requires progressive mechanical loading to stimulate tendon remodelling. [6]
Calcific Tendinosis

Calcium hydroxyapatite deposits form within the rotator cuff tendon, most commonly the supraspinatus. In the resorptive phase, these deposits can cause severe, acute shoulder pain disproportionate to apparent injury. Extracorporeal shockwave therapy has demonstrated significant improvements in pain and function in recent meta-analysis across 16 RCTs. [7]
Rotator Cuff Tears

Partial or full-thickness tears can be traumatic (sudden high force in younger individuals) or degenerative (moderate force in middle-aged and older adults). Full-thickness tears of the supraspinatus result in significant weakness with shoulder abduction. Importantly, not all tears require surgery, many partial tears and even full-thickness tears in older, lower-demand individuals respond well to conservative rehabilitation. [8]
Frozen Shoulder (Adhesive Capsulitis)

Frozen shoulder affects approximately 2–5% of the general population, with higher prevalence in people with diabetes and thyroid conditions. The joint capsule becomes inflamed and then progressively contracts, reducing range of motion in all directions, particularly external rotation and overhead reach. It proceeds through three stages: [11]
Freezing phase (2–9 months): Gradual onset of pain and progressive loss of motion. Often the most painful stage. Many patients are still seeking a diagnosis at this point.
Frozen phase (4–12 months): Stiffness plateaus. Pain may partially reduce but motion remains severely restricted. Daily function is significantly affected.
Thawing phase (5–24 months): Gradual, spontaneous return of motion. Without intervention, this phase can take over a year to complete.
The most effective conservative approach combines intra-articular corticosteroid injection in the early freezing phase with guided manual therapy and exercise. A 2024 systematic review found that combining intra-articular injection with physiotherapy produced faster restoration of range of motion than either intervention alone. [11]
Scapular Dyskinesis and Poor Shoulder Mechanics
Scapular dyskinesis, altered positioning or motion of the scapula during arm movement, is one of the most underdiagnosed drivers of shoulder pain. A 2018 systematic review and meta-analysis found that athletes with asymptomatic scapular dyskinesis are at 43% increased risk for developing shoulder pain within 24 months. [3]
The most common contributors include tightness of the pectoralis minor, weakness of the serratus anterior and lower trapezius, and restricted thoracic spine mobility. Current evidence emphasises that rehabilitation should focus primarily on enhancing motor control rather than simply increasing strength, restoring the precise timing and sequencing of scapular muscle activation, not just the force output. [2]
Visible signs include scapular winging (the medial border or inferior angle lifts away from the ribcage), shoulder blade asymmetry at rest, and poor quality overhead mechanics, hitching, shrugging, or early trunk side-bend during arm elevation.
Shoulder Instability and Labral Injuries
The shoulder is the most mobile joint in the body and that mobility comes at the inherent cost of stability. The labrum is a fibrocartilaginous ring that deepens the glenoid socket and provides the humeral head with a stable seating surface. It also serves as the attachment point for the glenohumeral ligaments.
Anterior dislocation (the most common type), tears the anterior labrum (a Bankart lesion) and stretches the anterior capsule and glenohumeral ligaments. If these structures do not heal, the shoulder becomes prone to recurrence with progressively less force required. Repeated instability can lead to progressive cartilage damage and early glenohumeral osteoarthritis.
Labral tears can also occur without dislocation, through repetitive overhead loading in swimmers, throwers, and weightlifters. SLAP tears (superior labrum anterior to posterior) are common in overhead athletes and can cause deep, poorly-localised shoulder pain, clicking, and a sense of instability with certain movements.
Unlike most shoulder conditions, instability typically responds better to targeted strengthening of the rotator cuff and dynamic stabilisers than to rest alone. The right exercise selection matters considerably, and premature return to overhead or throwing activity before adequate neuromuscular control is restored is one of the most common reasons instability recurs.
How Shoulder Pain Is Properly Assessed

A thorough shoulder assessment is the foundation of effective treatment. Without it, the risk of misdiagnosis and therefore misdirected treatment is high. A comprehensive shoulder evaluation should include the following.
Postural and Static Analysis
Assessment begins before any movement. The examiner observes head position, cervical lordosis, thoracic kyphosis, shoulder blade position and symmetry at rest, and overall spinal alignment. Many shoulder problems have an immediately visible postural component, forward head carriage, rounded shoulders, anteriorly tilted scapulae that must be addressed as part of the treatment plan.
Range of Motion Testing
Both active (patient-generated) and passive (examiner-guided) range of motion are assessed in all planes: flexion, abduction, internal and external rotation, horizontal adduction, and extension. The quality, arc, and pattern of movement are as important as the numbers. A painful arc between 60–120 degrees of abduction suggests impingement; global restriction in all planes suggests frozen shoulder; apprehension with specific movements suggests instability.
Scapulohumeral Rhythm Assessment
The examiner observes the scapula through a full arc of arm elevation, looking for timing, symmetry, winging, tipping, or early elevation. This is one of the most clinically informative parts of the shoulder assessment and one of the most commonly skipped in general practice.
Orthopedic and Special Tests
A battery of validated provocative tests helps identify the involved structure. Key tests include:
Hawkins-Kennedy and Neer tests - subacromial impingement
Empty Can and Full Can tests - supraspinatus integrity
External rotation lag sign - infraspinatus and teres minor
Lift-off and Belly Press tests - subscapularis integrity
Apprehension and Relocation tests - anterior glenohumeral instability
O'Brien's Active Compression test - labral pathology and AC joint
Speed's test - biceps long head tendinopathy
Posterior shoulder tightness assessment - posterior capsule involvement
Strength and Neuromuscular Control
Manual muscle testing of the rotator cuff, deltoid, serratus anterior, and trapezius quantifies strength deficits and identifies neuromuscular inhibition patterns. These findings directly inform exercise prescription.
Kinetic Chain Assessment
Core stability testing, hip mobility assessment, and thoracic rotation testing are included in a comprehensive shoulder evaluation because shoulder mechanics cannot be properly understood in isolation from the system that supports them.
Imaging
Imaging plays an important supporting role but should follow, not replace, a clinical assessment. Plain X-ray rules out fractures, assesses AC joint integrity, and identifies calcific deposits. Diagnostic ultrasound allows real-time assessment of rotator cuff tendons, bursa, and biceps. MRI provides the most comprehensive assessment of soft tissue structures and is indicated when a labral tear, full-thickness rotator cuff tear, or significant capsular pathology is suspected.
What Actually Helps: The Full Treatment Spectrum
Shoulder pain treatment is not one-size-fits-all. The right approach depends on the diagnosis, the stage of the condition, the patient's age and activity level, and how the condition has responded to previous care. Below is the full spectrum; from conservative first-line options through to surgical intervention.
Conservative Care: First-Line and Most Effective for Most Conditions
Chiropractic and Manual Therapy
Targeted joint manipulation and mobilisation of the glenohumeral joint, acromioclavicular joint, and critically; the thoracic spine and cervical spine reduces pain, restores joint mobility, and creates the window in which exercise-based rehabilitation can be performed more effectively. A 2024 systematic review and meta-analysis found that while manual therapy alone provides limited benefit, manual therapy combined with exercise or multimodal physiotherapy significantly reduces pain and enhances shoulder function in rotator cuff injury patients. [14]
A further 2024 living systematic review confirmed trustworthy evidence for manual therapy interventions in shoulder dysfunction, particularly when integrated with active rehabilitation. Thoracic manual therapy specifically has demonstrated positive effects on pain, disability, range of motion, and quality of life in subacromial pain syndrome patients across seven RCTs in a 2025 systematic review. [17]
Osteopathic Treatment
Osteopathy addresses the shoulder complex through a whole-body lens, assessing and treating the thorax, rib cage, and cervical spine as contributors to shoulder dysfunction. A 2024 comprehensive mapping review documented the wide range of documented biological effects following osteopathic manipulative treatment, including neurological, circulatory, and musculoskeletal responses. For frozen shoulder specifically, osteopathic approaches that include Spencer technique mobilisation and manipulation under anaesthesia have demonstrated improvements in range of motion and function. [21]
Soft Tissue Therapy
Active Release Technique (ART), myofascial release, and instrument-assisted soft tissue mobilisation (IASTM) address muscle and tendon adhesions, reduce tissue tension, and restore normal movement patterns. Particularly effective for pectoralis minor tightness, posterior shoulder tightness, and rotator cuff tendinopathy where fascial restrictions contribute to altered scapular mechanics.
Acupuncture and Dry Needling
A 2024 meta-analysis of 13 RCTs found that acupuncture combined with exercise rehabilitation produced significantly better outcomes for rotator cuff disease than exercise alone, corticosteroid injection alone, or sham acupuncture with improvements across pain, function, and range of motion. [18]
For dry needling specifically, a 2025 systematic review and meta-analysis found that dry needling combined with exercise reduced pain more than exercise alone across tendinopathy presentations including rotator cuff tendinopathy. A 2022 systematic review confirmed effectiveness for dry needling in subacromial syndrome. [19]
Exercise-Based Rehabilitation
Progressive, targeted loading is the most evidence-supported treatment for rotator cuff tendinopathy, scapular dyskinesis, and shoulder instability. The 2025 JOSPT Clinical Practice Guideline on rotator cuff tendinopathy provides the current gold standard for exercise prescription, including guidance on load, frequency, progression, and return to sport. Exercise rehabilitation should progress through three stages: pain-free range of motion restoration, scapular stabilisation and rotator cuff motor control, and progressive loading with functional integration. [6]

Shockwave Therapy
Extracorporeal shockwave therapy (ESWT) is well-evidenced for calcific tendinosis and chronic rotator cuff tendinopathy. A 2024 systematic review and meta-analysis across 16 RCTs demonstrated that ESWT produced significant improvements in pain (VAS) and function (Constant-Murley Score) compared to control interventions. [7]
Injection Therapies
Corticosteroid Injections
Subacromial corticosteroid injections can provide meaningful short-term pain reduction for impingement and bursitis, creating a window for rehabilitation that might otherwise be limited by pain. However, evidence shows that repeated corticosteroid injection has a negative long-term effect on tendon tissue and does not address the underlying mechanical drivers. It is a temporising measure, not a treatment strategy.
Platelet-Rich Plasma (PRP)
PRP involves concentrating a patient's own platelets from a blood draw and injecting them into damaged tissue to stimulate healing. A systematic review found PRP produces clinically meaningful improvements in shoulder pain and function for rotator cuff tendinopathy, with effects that appear more durable than corticosteroid injection in the medium to long term. PRP is increasingly offered as an alternative to surgery for patients with partial tears who have not responded to conservative care. [8]
Hydrodilatation (Distension Arthrography)
A procedure used specifically for frozen shoulder, injecting a large volume of saline, local anaesthetic, and corticosteroid into the joint capsule to stretch and break down adhesions. The 2024 Ochsner Journal review found that hydrodilatation combined with physiotherapy offers additive benefits for range of motion recovery, particularly when used alongside other conservative approaches. [12]
Hyaluronic Acid Injections
Used primarily for glenohumeral osteoarthritis, hyaluronic acid injections reduce pain and improve joint mobility by supplementing natural joint fluid. Benefit is modest in isolation but can support rehabilitation in older patients with combined degenerative and mechanical shoulder pathology.
Surgical Options
Surgery is appropriate for a minority of shoulder conditions, typically when conservative care has been adequately trialled and the structural problem cannot be resolved without intervention.
Arthroscopic Subacromial Decompression
This procedure was once among the most commonly performed shoulder surgeries. The landmark CSAW trial (Beard et al., 2018, Lancet), a multicentre, placebo-controlled trial across 32 UK hospitals, found no significant difference in outcomes between arthroscopic subacromial decompression, sham surgery, and no treatment at 12 months. A subsequent systematic review with meta-analysis confirmed high-certainty evidence of no additional benefit over placebo surgery. Current evidence reserves this procedure for cases with significant structural narrowing confirmed on imaging that have failed adequate rehabilitation. [9]
Rotator Cuff Repair
Surgical reattachment of torn rotator cuff tendons is indicated for full-thickness tears in younger, active patients or large tears causing significant functional limitation. Outcomes are good when followed by structured, progressive rehabilitation over 4–6 months. The current CPG emphasises that even full-thickness tears in lower-demand patients may be appropriately managed conservatively. [6]
Labral Repair (Bankart Repair)
Arthroscopic reattachment of the torn anterior labrum to the glenoid rim is the standard of care for young, active patients with recurrent anterior shoulder instability. Failure to address this surgically in high-demand patients risks progressive cartilage damage and early glenohumeral osteoarthritis.
Shoulder Replacement (Arthroplasty)
Total or reverse shoulder arthroplasty is indicated for severe glenohumeral osteoarthritis or for massive, irreparable rotator cuff tears in older patients. Outcomes have improved significantly with modern implant design, and post-operative rehabilitation is a critical determinant of functional outcome.
A note on surgery
Most shoulder conditions do not require surgery. The evidence consistently shows that well-delivered conservative care, combining manual therapy, guided exercise, and appropriate load management, produces outcomes equivalent to surgery for many rotator cuff and impingement presentations. Surgery is most clearly indicated for full instability with labral disruption, full-thickness tears in younger active patients, and end-stage arthritis.
Recovery Through the Four Pillars
At ONE80 Health, we assess and manage shoulder pain within a broader framework called the Four Pillars of Health; Movement, Nutrition, Sleep, and Mindset. These are not peripheral lifestyle factors. They are the physiological inputs that determine how fast tissue heals, how well the nervous system down-regulates pain, and whether a recovery holds over time.
Movement
The most important principle in shoulder recovery is that movement is medicine but it must be the right movement at the right load at the right time. Prolonged rest leads to capsular tightening, rotator cuff deconditioning, and neuromuscular inhibition. The 2025 JOSPT CPG recommends exercise therapy as the cornerstone of rotator cuff tendinopathy management, with a strong recommendation for progressive loading protocols. [6]
Rehabilitation must address the full kinetic chain, not just the shoulder. Thoracic spine mobility, core stability, and hip function all contribute to shoulder mechanics. A rehabilitation program that treats only the endpoint of the chain will consistently underdeliver.
Nutrition
Tendon and connective tissue have poor vascularity relative to muscle, which is part of why rotator cuff injuries take longer to heal and why nutritional status during recovery matters. Vitamin C-enriched gelatin supplementation taken 30–60 minutes before exercise has been shown to double circulating markers of collagen synthesis compared to placebo in a randomised crossover trial. [23]
A systematic review of collagen peptide supplementation found consistent evidence for improved joint recovery and connective tissue remodelling when combined with mechanical loading. Anti-inflammatory dietary patterns, rich in omega-3 fatty acids, polyphenols, and whole foods that support the resolution phase of healing. [24]
Vitamin C specifically plays a cofactor role in collagen synthesis through hydroxylation of proline and lysine residues, and a 2022 scoping review concluded that vitamin C supplementation increases collagen synthesis with consequent improvement in tendinopathy recovery. [25]
Sleep
Night pain is one of the most disruptive features of shoulder conditions, particularly rotator cuff tendinopathy, frozen shoulder, and bursitis. Lying on the affected side compresses the subacromial space and irritates sensitised tissue. Disrupted sleep elevates cortisol, increases central sensitisation, and raises pain perception the following day, creating a cycle that can significantly prolong recovery.
Positioning strategies make a meaningful difference. Sleeping on the unaffected side with a pillow supporting the affected arm in a neutral position reduces subacromial compression. Slightly reclined positioning reduces joint compression during the frozen phase. Avoiding overhead reaches in the first moments of waking protects the joint when it is least prepared for load.
Sleep quality is a clinical priority, not a secondary concern. It is when inflammation resolves, the nervous system down-regulates, and tissue repair accelerates.
Mindset
Fear-avoidance, restricting movement and activity because of anxiety about making injury worse; is one of the strongest independent predictors of poor outcomes in musculoskeletal conditions. The fear-avoidance model, established by Vlaeyen and Linton, describes how pain-related fear drives escape and avoidance behaviour, hypervigilance, protective muscle guarding, and physical deconditioning; all of which amplify pain and delay recovery. [26]
A 2007 review confirmed that fear-avoidance is an essential feature of chronic pain development across musculoskeletal conditions. For upper extremity pain specifically, a 2023 study found that high fear-avoidance beliefs are associated with poorer adherence to exercise programs and worse functional outcomes. [28]
This is not about pushing through pain. It is about understanding the difference between pain that signals genuine tissue threat and pain that reflects a sensitised nervous system. Education reduces fear. Reduced fear reduces pain. Confident, guided movement within appropriate limits accelerates recovery, consistently, across every shoulder condition we treat.
Breathing-based nervous system regulation; slow, exhale-dominant breathing for 3–5 minutes, directly reduces sympathetic tone and protective muscle guarding around the shoulder and neck. It is a simple, evidence-based tool that costs nothing and has no downside.
When to Seek Help
Most shoulder pain will not resolve on its own without some form of intervention and waiting typically allows compensatory patterns to become entrenched, making recovery longer and more complex.
The 3–10 day rule
If your shoulder symptoms are not improving or are getting worse; within 3 to 10 days of onset, get assessed. That is the window where early intervention makes the biggest difference. Waiting weeks or months is rarely in your interest.
Seek assessment promptly if you experience any of the following:
Pain that is not improving after 3–10 days, or that is progressively worsening
Significant loss of range of motion in multiple directions
Weakness with lifting or carrying that was not present before
A specific traumatic event; fall, collision, or forceful overhead reach
Numbness, tingling, or radiating pain down the arm into the hand
Night pain severe enough to consistently disrupt sleep
A sense of the shoulder 'giving way' or feeling unstable
The ONE80 Approach to Shoulder Pain
At ONE80 Health, shoulder pain is assessed and treated as a system problem, not a single joint problem. Our clinical team integrates chiropractic, osteopathy, acupuncture, and functional rehabilitation to address what is actually driving the condition, not just where it hurts.
Every shoulder patient at ONE80 receives a thorough assessment that includes postural analysis, scapulohumeral rhythm evaluation, orthopedic testing, kinetic chain assessment, and a clear diagnosis and treatment rationale before any hands-on care begins.
Treatment plans are built around the Four Pillars framework, ensuring that the clinical work in the office is supported by the right habits and inputs at home. We work with patients on movement, nutrition, sleep positioning, and mindset in parallel with hands-on care because that is what produces durable outcomes.
Ready to get your shoulder properly assessed?
Same-day and next-day appointments available. Our team will identify what's driving the pain and build a clear plan for recovery.
References
All references link directly to PubMed or the publisher source. Inline citation numbers correspond to the bracketed superscripts throughout the post.
[1] Longo UG et al. Scapular Dyskinesis: From Basic Science to Ultimate Treatment. Int J Environ Res Public Health. 2020;17(8):2974. https://pubmed.ncbi.nlm.nih.gov/32344746/
[2] Sciascia A, Kibler WB. Current Views of Scapular Dyskinesis and its Possible Clinical Relevance. Int J Sports Phys Ther. 2022;17(2):117-130. https://pubmed.ncbi.nlm.nih.gov/35136680/
[3] Hickey D et al. Scapular dyskinesis increases the risk of future shoulder pain by 43% in asymptomatic athletes: a systematic review and meta-analysis. Br J Sports Med. 2018;52:102-110. https://pubmed.ncbi.nlm.nih.gov/28870962/
[4] Kibler WB, Sciascia A. Evaluation and Management of Scapular Dyskinesis in Overhead Athletes. Curr Rev Musculoskelet Med. 2019;12(4):515-526. https://pubmed.ncbi.nlm.nih.gov/31760624/
[5] Leong HT et al. Risk factors for rotator cuff tendinopathy: A systematic review and meta-analysis. J Rehabil Med. 2019;51(9):627-637. https://pubmed.ncbi.nlm.nih.gov/31334563/
[6] Beneciuk JM et al. Rotator Cuff Tendinopathy Diagnosis, Nonsurgical Medical Care, and Rehabilitation: A Clinical Practice Guideline. J Orthop Sports Phys Ther. 2025;55(4):235-274. https://www.jospt.org/doi/10.2519/jospt.2025.13182
[7] Xue X et al. Effect of extracorporeal shockwave therapy for rotator cuff tendinopathy: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2024;25(1):357. https://pubmed.ncbi.nlm.nih.gov/38704572/
[8] Nazari G et al. Platelet-rich plasma for rotator cuff tendinopathy: A systematic review and meta-analysis. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/33970936/
[9] Beard DJ et al. Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, placebo-controlled, three-group, randomised surgical trial. Lancet. 2018;391(10118):329-338. https://pubmed.ncbi.nlm.nih.gov/29169668/
[10] Karjalainen TV et al. Subacromial decompression surgery for adults with shoulder pain: a systematic review with meta-analysis. Br J Sports Med. 2019;54(11):665-673. https://pubmed.ncbi.nlm.nih.gov/30647053/
[11] Li D, St Angelo JM, Taqi M. Adhesive capsulitis (frozen shoulder). StatPearls. 2025. PMID: 40095380. https://pubmed.ncbi.nlm.nih.gov/40095380/
[12] Hill JL et al. Evidence for Combining Conservative Treatments for Adhesive Capsulitis. Ochsner J. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10949050/
[13] Tafler M et al. The Function of Osteopathic Medicine in the Treatment of Adhesive Capsulitis. Cureus. 2022;14(8):e27862. https://pubmed.ncbi.nlm.nih.gov/36072175/
[14] Liu S et al. Efficacy of manual therapy on shoulder pain and function in patients with rotator cuff injury: A systematic review and meta-analysis. Biomed Rep. 2024;20(6):89. https://pubmed.ncbi.nlm.nih.gov/38682089/
[15] Flowers DW et al. Is there 'trustworthy' evidence for using manual therapy to treat patients with shoulder dysfunction? A systematic review. PLoS One. 2024;19(1):e0297234. https://pubmed.ncbi.nlm.nih.gov/38236928/
[16] Paraskevopoulos E et al. Effectiveness of combined program of manual therapy and exercise vs exercise only in patients with rotator cuff-related shoulder pain: A systematic review and meta-analysis. Sports Health. 2023;15(2):176-186. https://pubmed.ncbi.nlm.nih.gov/36517977/
[17] Thoracic Manual Therapy With or Without Exercise Improves Pain and Disability in Subacromial Pain Syndrome: A Systematic Review. Healthcare. 2025;13(19):2479. https://www.mdpi.com/2227-9032/13/19/2479
[18] Zhang HN et al. Efficacy comparison between acupuncture and other modalities in the treatment of rotator cuff diseases: meta-analysis of RCTs. Am J Transl Res. 2024;16(2):599-616. https://pubmed.ncbi.nlm.nih.gov/38463603/
[19] Pourshafie T et al. Effectiveness of Dry Needling Combined With Exercise Versus Exercise Alone in Various Tendinopathies: A Systematic Review and Meta-Analysis. PMC. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12538665/
[20] Blanco-Diaz M et al. A Systematic Review of the Effectiveness of Dry Needling in Subacromial Syndrome. Biology. 2022;11(2):243. https://pmc.ncbi.nlm.nih.gov/articles/PMC8869493/
[21] Dal Farra F et al. Reported biological effects following Osteopathic Manipulative Treatment: A comprehensive mapping review. Complement Ther Med. 2024;82:103043. https://pubmed.ncbi.nlm.nih.gov/38685285/
[22] Pieters L et al. An Update of Systematic Reviews Examining the Effectiveness of Conservative Physical Therapy Interventions for Subacromial Shoulder Pain. J Orthop Sports Phys Ther. 2020;50(3):131-141. https://pubmed.ncbi.nlm.nih.gov/31726927/
[23] Shaw G et al. Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis. Am J Clin Nutr. 2017;105(1):136-143. https://pubmed.ncbi.nlm.nih.gov/27852613/
[24] Morton RW et al. The effects of collagen peptide supplementation on body composition, collagen synthesis, and recovery from joint injury and exercise: a systematic review. PMC. 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8521576/
[25] Fusini F et al. Effect of Vitamin C on Tendinopathy Recovery: A Scoping Review. Nutrients. 2022;14(13):2642. https://pubmed.ncbi.nlm.nih.gov/35807843/
[26] Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317-332. https://pubmed.ncbi.nlm.nih.gov/10781906/
[27] Leeuw M et al. The Fear-Avoidance Model of Musculoskeletal Pain: Current State of Scientific Evidence. J Behav Med. 2007;30(1):77-94. https://pubmed.ncbi.nlm.nih.gov/17180640/
[28] Navarro-Santana MJ et al. Fear Avoidance Beliefs in Upper-Extremity Musculoskeletal Pain Conditions. PubMed. 2023. PMID: 36200858. https://pubmed.ncbi.nlm.nih.gov/36200858/
[29] Manual therapy and exercise for adhesive capsulitis: a systematic review with meta-analysis. PubMed. 2023. PMID: 36861780. https://pubmed.ncbi.nlm.nih.gov/36861780/